The efficacy of Bosentan has not been established in patients with severe PAH. Transfer to a therapy that is recommended at the severe stage of the disease (e.g. Epoprostenol) should be considered if the clinical condition deteriorates.
The benefit/risk balance of Bosentan has not been established in patients with WHO class I functional status of PAH.
Bosentan should only be initiated if the systemic systolic blood pressure is higher than 85 mmHg.
Bosentan has not been shown to have a beneficial effect on the healing of existing digital ulcers.
Liver function: Elevations in liver aminotransferases, i.e. aspartate and alanine aminotransferases (AST and/or ALT), associated with Bosentan are dose dependent. Liver enzyme changes typically occur within the first 26 weeks of treatment but may also occur late in treatment. These increases may be partly due to competitive inhibition of the elimination of bile salts from hepatocytes but other mechanisms, which have not been clearly established, are probably also involved in the occurrence of liver dysfunction. The accumulation of Bosentan in hepatocytes leading to cytolysis with potentially severe damage of the liver, or an immunological mechanism, are not excluded. Liver dysfunction risk may also be increased when medicinal products that are inhibitors of the bile salt export pump, e.g. Rifampicin, Glibenclamide and Cyclosporine A, are co-administered with Bosentan, but limited data are available. (See Table 2.)
 Click on icon to see table/diagram/image
Hemoglobin concentration:
Click on icon to see table/diagram/image
Hemoglobin concentration: Treatment with Bosentan has been associated with dose-related decreases in hemoglobin concentration. It is recommended that hemoglobin concentrations be checked prior to initiation of treatment, every month during the first 4 months, and quarterly thereafter. If a clinically relevant decrease in hemoglobin concentration occurs, further evaluation and investigation should be undertaken to determine the cause and need for specific treatment.
Pulmonary veno-occlusive disease: Cases of pulmonary edema have been reported with vasodilators (mainly prostacyclins) when used in patients with pulmonary veno-occlusive disease. Consequently, should signs of pulmonary edema occur when Bosentan is administered in patients with PAH, the possibility of associated veno-occlusive disease should be considered.
Pulmonary arterial hypertension patients with concomitant left ventricular failure: Treatment with diuretics should be considered in patients with evidence of fluid retention before the start of treatment with Bosentan.
Pulmonary arterial hypertension associated with HIV infection: An increased long-term risk of hepatic toxicity and hematological adverse events cannot be excluded when Bosentan is used in combination with antiretroviral medicinal products. Due to the potential for interactions related to the inducing effect of Bosentan on CYP450, which could affect the efficacy of antiretroviral therapy, these patients should also be monitored carefully regarding their HIV infection.
Pulmonary hypertension secondary to chronic obstructive pulmonary disease (COPD): An increase in minute ventilation and a decrease in oxygen saturation were observed, and the most frequent adverse event was dyspnea, which resolved with discontinuation of Bosentan.
Concomitant use with other medicinal products: Concomitant use of Bosentan and Cyclosporine A is contraindicated.
Concomitant use of Bosentan with Glibenclamide, Fluconazole and Rifampicin is not recommended.
Concomitant administration of both a CYP3A4 inhibitor and a CYP2C9 inhibitor with Bosentan should be avoided.
Women of childbearing potential: As Bosentan may render hormonal contraceptives ineffective and taking into account the risk that pulmonary hypertension deteriorates with pregnancy: Bosentan treatment must not be initiated in women of childbearing potential unless they practice reliable contraception and the result of the pre-treatment pregnancy test is negative.
Hormonal contraceptives cannot be the sole method of contraception during treatment with Bosentan.
Monthly pregnancy tests are recommended during treatment to allow early detection of pregnancy.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image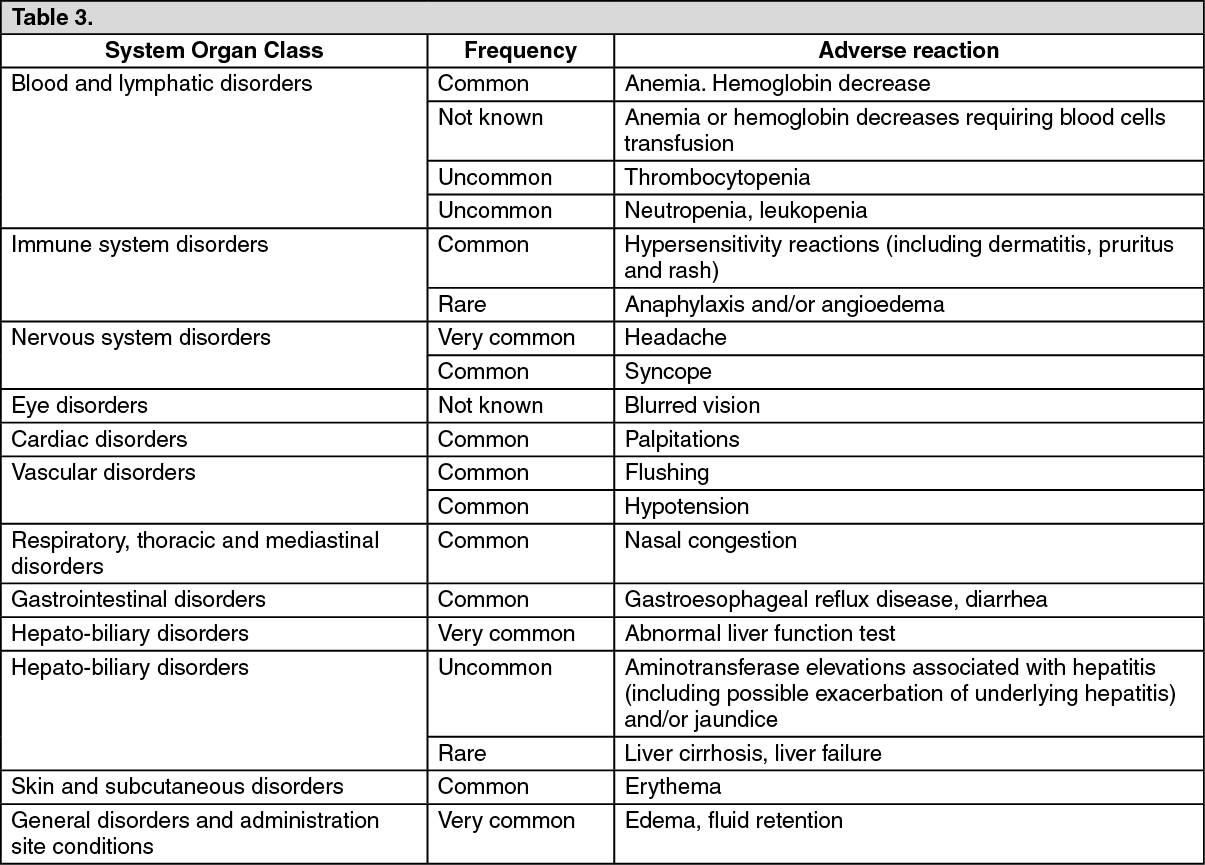 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
